Birth Injury

Pelvic Organ Prolapse Is More Common Than You Think — Here’s How I Finally Got Help For Mine
My body and I had a falling out.
“And that is your rectum,” said my pelvic floor therapist, whom I’d met just an hour earlier. Her tone was preternaturally calm, considering that she just informed me an organ was falling out of my body.
I was laying on her exam table with my legs in the stirrup position while she held a mirror up (or rather, down) to my vagina so I could see exactly what she was referring to. She had asked me to bear down as I had while giving birth to my son, and that’s when I saw it. It looked a bit like a uvula, that freaky little thing that hangs down in the back of your throat.
“That’s my rectum?!” I heard the words coming out of my mouth in shock. I was never a particularly shy person when it came to my body, but I had become pretty disconnected from the neck down since having my two children. I had delivered one vaginally and the other via C-section, but my kids were 4 and 7 by then, so it had been a while since I had taken a good look down there.
Turns out that in addition to having split my abs (aka diastasis recti) during my first pregnancy and suffering a third-degree tear during my son’s birth because he had to be vacuumed out, my pelvic floor had become so weak that my rectum was literally falling out of my body. I could see it with my own eyes in that mirror. As I lay my head back on the exam table, I was hit by a tidal wave of disbelief, shame, and panic. Why — how! — did I not know about this sooner? Why did my gynecologist never mention this to me? Would I have to get surgery? Was this even normal?
“There’s no official screening for prolapsed organs after childbirth. It’s almost as if it’s a luxury to maintain bodily function.”
It has taken me a while to get answers to these questions. After the initial diagnosis of “rectocele” or a posterior vaginal prolapse, wherein your rectum bulges into your vagina, I have spent a year in physical therapy to rebuild the parts of my body that felt broken beyond repair, and months in cognitive behavioral therapy to overcome the ensuing shame. I wanted to understand how and why organ prolapse of the bladder, uterus, and rectum happens to women after childbirth, and share what I’ve learned so other women can recover from this, too.
Some women don’t experience any symptoms from their pelvic organ prolapse, but many more are not able to connect the dots between a symptom and their injured pelvic floor. That might be different if pelvic floor screening was a routine part of postpartum care. “There’s no official screening for prolapsed organs after childbirth. It’s almost as if it’s a luxury to maintain bodily function,” says Dr. Tirsit Asfaw, M.D., a urogynecologist at Weill Cornell in New York City, who has devoted her career to helping women restore not just their pelvic floor strength and function, but also their confidence in their bodies. “Unfortunately, that’s what society has done to women.”
Looking back years later, I am bewildered as to why the very doctor who did a cavity search of my vagina regularly for nine months didn’t take a peek inside after I pushed out a 7-pound baby to tell me whether one of my organs was falling out. Especially since I had a third-degree tear, increasing the likelihood that I would have severe pelvic floor damage.
Instead, at my six-week postpartum appointments, my OB-GYN cleared me for the two least appealing activities a sleep-deprived new parent can imagine: exercise and sex. “The six-week checkup is to ensure you’re medically stable — to say you’re not hemorrhaging, we don’t think you’re going to have a stroke,” says Leah Keller, a certified personal trainer and co-founder of Every Mother, a platform that provides exercise programs for abdominal separation and pelvic floor dysfunction. “It is to make sure we think you’re going to survive.”

Though urogynecologists have been advocating for years to screen for pelvic floor disorders at that six-week postpartum appointment — to ask about incontinence, vaginal pain, and bowel movements — the American health care system is apparently not set up to accommodate this. “Insurance companies allow for 15-minute appointments, which doesn’t give the OB enough time to evaluate your pelvic floor,” says Keller.
Despite the fact that I have always been health-conscious and used to work at women’s health magazines, I never came across any information about pelvic floor health before my own diagnosis. My female co-workers who were pregnant and postpartum never mentioned it, even as we were working on magazine stories about taking care of your body. We edited countless stories about how to tighten your abs, and zero about the pelvic floor or what happens to it after childbirth.
Think of all the times you’ve heard a mother toss off an aside like “I have to cross my legs when I sneeze!” or “I can’t run without peeing a little!” What they — and I — did not realize is that these symptoms suggest a prolapsed bladder. Not only is it not funny to pee when you’re doing normal activities, but there are plenty of women who experience straining while going to the bathroom (indicating a prolapsed rectum) and painful sex (35% of women report pain with intercourse after childbirth).
For years after my children were born, I simply tolerated the symptoms.
Whether or not you experienced postpartum mental health conditions — I had severe postpartum anxiety, OCD, and depression after I gave birth to my son in 2016 — so many women are too overwhelmed with mothering (and working, if you have a job) to think about whether their pelvic floor is damaged after birth. We prioritize our baby’s doctor appointments and child care over our own health and well-being, especially in the beginning, when pelvic floor therapy would be most effective in preventing a prolapse. (Though not, it should be noted, too soon. Experts agree that initial rest and healing are necessary postpartum and most doctors recommend starting after the six-week mark.)
For years after my children were born, I simply tolerated the symptoms. The first mortifying sign showed up when I began to do yoga again. Every time I opened my body into a Warrior 2 or Malasana squat, air would noisily squelch out of my nether regions (how Zen!). And when sex hurt because of the scar tissue that had formed in my vagina where I tore, my OB-GYN told me that was “normal” and that it would soften and hurt less the more I had intercourse. (This so-called medical “advice” now enrages me.)
In the end — as is the case with many women — it was another body part entirely that tipped me off to my prolapse. I kept pinching a nerve in my back, causing acute pain that prevented me from turning my head, never mind working out. My chiropractor recommended I see a physical therapist; she believed my core wasn’t properly supporting my body after birth. Turns out the extreme pain in my back was actually being caused by my diastasis recti. When your core becomes weak, sometimes your back muscles will overcompensate in an effort to do the work that your stomach no longer can, causing strain and pain. She recommended a pelvic floor therapist, who would be trained to work on my core as well as my pelvic floor.
I finally went for my first pelvic floor assessment in February 2020, right after my younger child turned 2. Weeks later, Covid lockdown happened. At that point I was only diagnosed with split abs and a weak pelvic floor — I had no idea about the prolapsed rectum yet. Two long years later, during which my pelvic floor further deteriorated and I experienced increasing back pain, I finally made it back to pelvic floor PT.

If you broke any other part of your body — let’s say you tore your Achilles tendon — your doctor would likely evaluate you and advise you to do physical therapy and potentially get surgery. But when you damage your pelvic floor, that is mysteriously not the case.
Finding a physical therapist who specializes in pelvic floor rehabilitation can be a major challenge. In the U.S., unlike in many countries in Europe, insurance doesn’t always cover pelvic floor PT and many practitioners are out of network. My search for a qualified pelvic floor therapist ultimately led me to Youstina Gerges, a doctor of physical therapy at Rise Above PT in Wyckoff, New Jersey. I had to travel an hour round trip to see her and she was not covered by my insurance, but I went anyway because I was desperate to relieve my pain. She had all the proper certifications, but most importantly she immediately made me feel comfortable.
After my first physical therapy appointment, I sat in the parking lot and sobbed in my car.
Gerges described my pelvic floor to me as a hammock of muscles that sits between your coccyx and pubic bone and supports your bladder, uterus, and rectum. She told me to imagine dropping a 7-pound (or 8- or 9-pound) bowling ball into that hammock, carrying it around for 40 weeks, and then pushing it out of your vagina or having it cut out of your abdomen. Pregnancy hormones also loosened my floor so that the baby could travel through my birth canal, so those ligaments and connective tissues were stretched up to three times their length during my first, vaginal delivery.
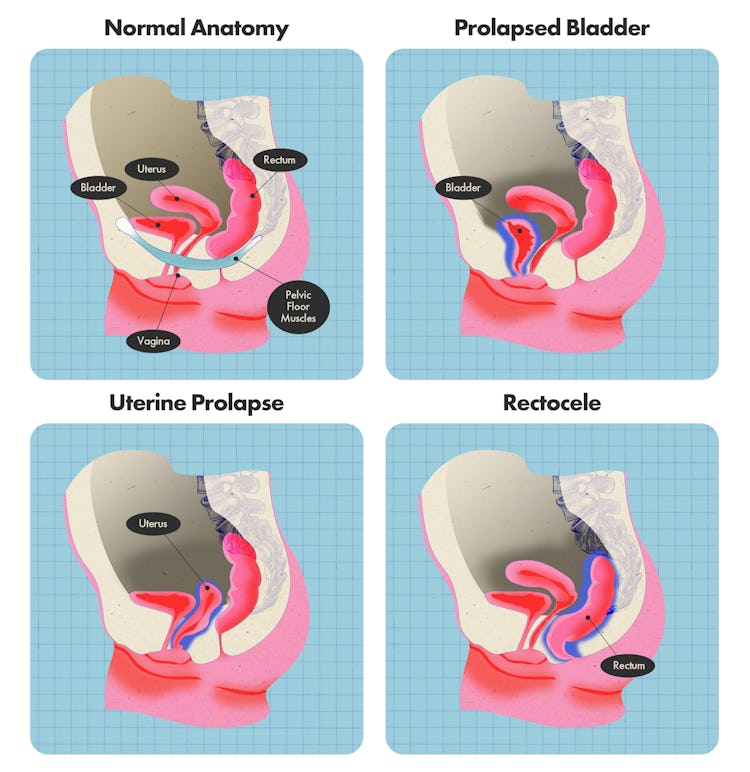
Prolapse happens when one of those three organs — or, in very rare cases, the intestines — shift from their normal positions in relation to your vagina. When your bladder bulges in, it’s called an anterior prolapse; when your uterus drops in, it’s called a uterine prolapse; a posterior wall prolapse is when your bowel protrudes into the rear wall of your vagina; and a vaginal vault prolapse is when the top of your vagina slips out of its position. Up to 50% of women experience prolapse in their life — not always because of childbirth — though one study found that a third of women who deliver vaginally will experience symptoms.
There are four stages of prolapse: in the first stage, your organ bulges into the upper half of your vagina; in the second, it hangs near the opening of your vagina; in the third, which is what I had, the organ protrudes out of your vagina; and in the fourth stage, the organ slips outside your vagina altogether. For some women, prolapse gets worse over time; for others, it will stay the same. There are many factors that contribute to whether a prolapse worsens. “Incorrect breathing patterns can push the organ lower,” says Gerges. Straining when using the bathroom is one example of breathing incorrectly. “Symptoms can also get worse with menopause.”
Research shows that if your prolapse is diagnosed and treated in the early postpartum period, it will get better within the first year after giving birth, but that 19% to 48% of women with a stage one or two prolapse will regress without intervention over three to eight years (that’s me!).
The first session with Gerges was particularly difficult for me, physically and emotionally. She began with a full-body evaluation: she assessed me externally, checking the muscles and joints in my back, spine, hips, and core, looking at mobility, flexibility, and strength. She felt my C-section scar to see how it had healed and to examine the scar tissue. And then, with my explicit permission, she examined me internally: she felt inside my vagina to assess the strength of my pelvic floor muscles — there are 26 of them — and to see if there were any knots, just as you might have knots in your back.
The early phase of my recovery was frustrating because it felt like I had to relearn basic functions.
I was surprised to learn that having “tight” pelvic muscles was not a good thing. Instead of meaning I would feel “tight” during sex, it meant those pelvic muscles had been traumatized and needed to be released and softened before I could actually strengthen them; a tight pelvic floor is actually a weak pelvic floor. This is also when she diagnosed the rectum prolapse.
After that first appointment, I sat in the parking lot and sobbed in my car. I also cried several times in her office during my initial sessions, coming to terms with what had happened to my body. During one particularly intense session when she was manually releasing my C-section scar, I broke down because I had still been holding on to so much shame that I couldn’t deliver my daughter vaginally. (I had been conditioned to think C-sections are a failure, which they most certainly are not.) The C-section had altered my body in irreversible ways. My stomach, formerly flat from decades of dancing, formed a shelf over my scar. I had compartmentalized that pain — and tolerated that I was never able to have an orgasm during sex after I had my daughter. Physical therapy became a place where I started to process the trauma.
I met with Gerges twice a week for six months for internal therapy, during which she manually released my pelvic floor muscles. She would talk me through which layer of pelvic muscles she was targeting — there are three that are each increasingly difficult to release. When she found a “knot,” it felt like she was sticking her finger in a wound, sometimes accompanied by a burning sensation. She was essentially doing myofascial trigger release inside my vagina. She explained that there are sensitive nerves in the pelvic floor, including the pudendal nerve, and they can become inflamed.
In those early sessions, she also taught me how to breathe diaphragmatically in order to properly re-engage my core and pelvic floor while doing simple activities like carrying my children. This phase was frustrating because it felt like I had to relearn basic functions.

My progress was slow, but after six months of regular PT, my pelvic floor muscles were strong enough to begin to restore my rectum to its place. I also began to notice other changes: learning how to breathe in a way that engaged my core and pelvic floor made a big difference when I was doing everyday activities like carrying grocery bags. I had to take it easy for a while with yoga, but over time I was able to start lifting weights again without throwing my back out. Generally, I became more aware of my pelvic floor and whether it was tense — I even started experiencing more sensitivity during sex. Ultimately, I had to stop seeing Gerges because the cost was prohibitive, but I found another pelvic floor physical therapist in my insurance network. She doesn’t do the internal work (not all PTs are certified) so she focuses on external ways I can release my tight pelvic floor muscles, as well as more challenging exercises that will strengthen my core and allow me to lift heavier weights as I get older.
When I was first diagnosed with a rectal prolapse, I thought surgery was inevitable. I was advised to see if PT would resolve the prolapse and pain first, which it mostly has. (Though I would still consider surgery if my condition deteriorated.) There are a lot of factors that go into how urogynecologists determine whether a woman with a prolapsed organ should get surgery. “It depends on what organ is falling out, how much is falling out,” Asfaw explains. “How old is the patient, do they want more children? It’s a longer discussion.” If you do want more children, a surgeon will probably advise you to wait because the next pregnancy and birth will stretch everything out again, says Asfaw.
At the price of my own discomfort, I now tell every mom I know who has mentioned “peeing while they run” or painful sex about pelvic floor rehab.
“I always advise conservative measures first,” Asfaw explains. “For a great majority of women, things may heal with physical therapy.” Often she will assess a patient, prescribe PT, and then reassess every three months to see if things are improving. If it is an extreme case — for example, a woman’s entire bladder empties every time she stands up — Asfaw will prioritize surgery.
One of the biggest roadblocks to getting the care so many women need is our shame around discussing certain bodily dysfunctions after birth. At the price of my own discomfort (socially and emotionally, that is), I now tell every mom I know who has mentioned “peeing while they run” or painful sex about pelvic floor rehab. I spent years suffering, and I wish someone had told me that I did not need to. Childbirth hurts; we’re supposed to be the warrior mothers who soldier through it. But I am done with that narrative and ready to rewrite it. “You have to go to hell and back to get the care you need,” says Asfaw. “Dealing with women’s health has never been the focus for our society and I hope that will change.”
But nothing will change if we don’t start advocating for ourselves, no matter how long it has been since you gave birth: “It’s never too late to restore your pelvic floor,” says Keller. “When you’re ready to commit, it’s the right time. Once postpartum, always postpartum.”
These days I use the Humpty Dumpty analogy to describe my pelvic floor recovery. Giving birth breaks you open physically and mentally in a million different amazing and painful ways that I wouldn’t trade for the world. The broken pieces are all different shapes and sizes, and you have to pick them up and learn how to put them back together. You become whole again, in a new way.
Cristina Tudino is a writer, editor, and content brand marketer. Her work has appeared in SELF, Health, Oprah, Women’s Health, Forbes.com, Martha Stewart Living, and Glamour. She is the founder of Gemini Consulting Group, and lives in New Jersey with her husband and two children.
